








 Buscar
Buscar
- Nuestro Centro
- Entorno asistencial Teknon
- Institutos de tratamiento especializado
- Campus TeknonEl área de Consultorios dispone de 2 edificios de consultas con 150 despachos médicos, con conexión directa con la clínica y acceso directo al parking.
- Especialidades
- Unidades especializadas
- Medicina y Cirugía sin sangre
- Reproducción Asistida
- Unidad de Atención al Lesionado de Tráfico
- Unidad de Enfermedades Inflamatorias y Autoinmunes
- Unidad de Epilepsia y Cirugía de Epilepsia
- Unidad de Medicina Marítima
- Unidad de Neumología
- Unidad de Obesidad
- Unidad de Obstrucción Respiratoria Nasal
- Unidad de Pediatría y Cirugía pediátrica
- Unidad de Síndromes de Sensibilización Central
- Unidad de Tratamiento del Dolor
- Unidad del Virus del Papiloma Humano
- Unidad del Aliento
- Unidad del Parkinson y Trastornos del movimiento
- Unidad del Sueño
- Especialidades
- Cardiología y Cirugía Vascular
- Cirugía general
- Cirugía estética
- Cirugía maxilofacial
- Clínica del Dolor
- Gastroenterología
- Ginecología y obstetricia
- Medicina Interna
- Neumología
- Neurología y Neurocirugía
- Oncología
- Otorrinolaringología
- Pediatría y cirugía pediátrica
- Traumatología
- Urología
- Todas las especialidades
- Localice un especialistaEn nuestro campus ejercen más de 400 especialistas de primera línea, con formación internacional en cada una de sus áreas y atención al paciente en varios idiomas.
- Unidades especializadas
- Área diagnóstica
 Diagnóstico cardiaco
Diagnóstico cardiaco
 Pruebas diagnósticas
Pruebas diagnósticas
 Chequeos médicos This link will open in a pop-up window.
Chequeos médicos This link will open in a pop-up window.- General This link will open in a pop-up window.
- Completo This link will open in a pop-up window.
- Completo Plus This link will open in a pop-up window.
- Viajeros This link will open in a pop-up window.
- Deportivo This link will open in a pop-up window.
- Cardiológico This link will open in a pop-up window.
- Empresa This link will open in a pop-up window.
- Exclusividad/Club Teknon
- La mejor atención
- La mejor asistencia
- Otros servicios
- Actualidad
- Comunicación
- AgendaPuedes encontrar todos los eventos que hemos organizado sobre salud y aquellos temas de actualidad que te pueden interesar. Accede a nuestra agenda de actividades.
- El Blog de Centro Médico TeknonLa salud, la ciencia y la medicina responden a la racionalidad, el empirismo, los resultados y las cifras. Pero, ¿qué hay de las personas? El factor humano es una parte esencial en la medicina que, algunas veces, queda en segundo plano. This link will open in a pop-up window.
Gilete Vicenç
Inestabilidad atlantoaxoidea
The surgical treatment for Atlantoaxial instability, when it manifests alone without occipitocervical instability, it mainly consists of a posterior fusion of the first cervical vertebra (C1 or Atlas) and the second cervical vertebra (C2 or Axis).
 In the Axis, pedicle screws are usually the first choice although, depending on the patient’s anatomy, placement of isthmic screws may be considered. Atlas’ screws are generally placed in the lateral masses. Atlas and axis screws are joined in each side by lateral bars that are unifying the instrumented fusion system. In most cases it is convenient to put bone graft, usually autologous, taken from the iliac crest or the patient’s own rib. In the cases where it is not possible to obtain autologous bone graft, heterologous graft (artificial bone) may also be used.
In the Axis, pedicle screws are usually the first choice although, depending on the patient’s anatomy, placement of isthmic screws may be considered. Atlas’ screws are generally placed in the lateral masses. Atlas and axis screws are joined in each side by lateral bars that are unifying the instrumented fusion system. In most cases it is convenient to put bone graft, usually autologous, taken from the iliac crest or the patient’s own rib. In the cases where it is not possible to obtain autologous bone graft, heterologous graft (artificial bone) may also be used.
When Atlantoaxial instability occurs along with craniocervical instability, also known as occipitocervical instability (ie instability present also between skull and first cervical vertebra or Atlas), then fusion should consist of adding a fixation to the cranial bone through occipital or condylar screws which would give us as a whole C0 -C1-C2 posterior fusion.
The personalized evaluation of each case is always convenient since it is very important that abnormalities of the vertebral artery anatomy are ruled out as well as the possible anatomical differences regarding the layout and dimensions of the vertebral pedicles, lateral masses and other bone elements.
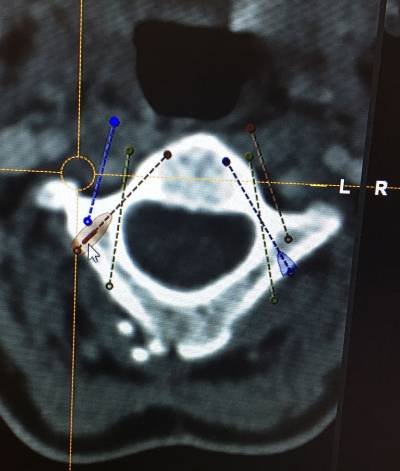
 After the preoperative analysis of the Magnetic Resonance Imaging (MRI) and CT scan of each patient, we perform a thin sliced preoperative CT oriented towards neuronavigation that will be carried out during surgery. Prior to surgery we perform a surgical planning of the intraoperative neuronavigation to confirm the trajectories of screws and special anatomical dispositions of structures. It is also important to know and evaluate patients’ concomitant diseases or comorbidities which are frequent in patients affected by Ehler Danlos, such as POTS, Mast Activation Syndrome, cardiac abnormalities … etc. Knowing this it allows to anticipate any possible problems in the postoperative period.
After the preoperative analysis of the Magnetic Resonance Imaging (MRI) and CT scan of each patient, we perform a thin sliced preoperative CT oriented towards neuronavigation that will be carried out during surgery. Prior to surgery we perform a surgical planning of the intraoperative neuronavigation to confirm the trajectories of screws and special anatomical dispositions of structures. It is also important to know and evaluate patients’ concomitant diseases or comorbidities which are frequent in patients affected by Ehler Danlos, such as POTS, Mast Activation Syndrome, cardiac abnormalities … etc. Knowing this it allows to anticipate any possible problems in the postoperative period.
Once in the Operating Room, surgery is performed under general anesthesia, with Neurophysiological monitoring (SSEP – somatosensory evoked potentials), neuronavigation guidance and intraoperative fluoroscopy guidance. Thus we control the spinal cord and nerves (cranial and cervical) in order to avoid potential damages to these important structures. Neuronavigation assistance guides us all through the surgery, thus it diminishes (though it does not eliminate) the risks while placing the screws for the fusion. Both neurophysiological monitoring and neuronavigation guidance are safety measures for the patient.
Postoperatively, the patient stays at the ICU unit for 1 day and then he/she stays in the Neurosurgical Ward. Postoperative hospital stay is usually around 7 days. Wake up and walking begins on the second day after surgery. After hospital discharge, doctors usually control patients at least once a week after discharge on an outpatient basis, to make sure everything is correct before flying back home, thus we recommend to stay in Barcelona after discharge for 10-15 days.
Fuentes:
- Dr. Vicenç Gilete, MD, Neurosurgeon &Spine Surgeon.
- Mummaneni PV, Haid RW. Atlantoaxial fixation: overview of all techniques. Neurol India. 2005 Dec;53(4):408-15. Review.
- Nuestro Centro
- Entorno asistencial Teknon
- Institutos de tratamiento especializado
- Campus Teknon
- Especialidades
- Unidades especializadas
- Especialidades
- Localice un especialista
- Área diagnóstica
- Exclusividad/Club Teknon
- La mejor atención
- La mejor asistencia
- Otros servicios
- Actualidad
- Comunicación
- Agenda
- El Blog de Centro Médico Teknon

Carrer de Vilana, 12, 08022 Barcelona
932 906 200