


- Medical directory
- Specialities
- Unidades especializadas
 Instituto del Corazón
Instituto del Corazón Unidad de Obesidad
Unidad de Obesidad Instituto Oncológico
Instituto Oncológico Unidad de Medicina y Cirugía sin sangre
Unidad de Medicina y Cirugía sin sangre Instituto de Neurociencias
Instituto de Neurociencias Unidad de Atención al Lesionado de Tráfico
Unidad de Atención al Lesionado de Tráfico Instituto de Neumología
Instituto de Neumología Unidad de Medicina Marítima
Unidad de Medicina Marítima Instituto de Terapia Regenerativa Tisular
Instituto de Terapia Regenerativa Tisular Unidad de Tratamiento del Dolor
Unidad de Tratamiento del Dolor Clínica del Tenis
Clínica del Tenis Unidad de Enfermedades Inflamatorias y Autoinmunes
Unidad de Enfermedades Inflamatorias y Autoinmunes Unidad de Reproducción
Asistida
Unidad de Reproducción
Asistida Unidad del Sueño
Unidad del Sueño Unidad de Síndromes de Sensibilización Central
Unidad de Síndromes de Sensibilización Central
- Unidades especializadas
- Diagnostics
- Diagnostic tests
 Diagnostic ImagingDiagnostic and interventional scans.
Diagnostic ImagingDiagnostic and interventional scans. Anatomical pathology laboratoryAllows to obtain a second opinion from renowned specialists.
Anatomical pathology laboratoryAllows to obtain a second opinion from renowned specialists. Clinical Analysis LaboratoryComprehensive service in the clinical area.
Clinical Analysis LaboratoryComprehensive service in the clinical area. EndoscopyAn accurate diagnosis without conventional surgery.
EndoscopyAn accurate diagnosis without conventional surgery. ElectrophysiologyFunctional exploration of the central nervous system.
ElectrophysiologyFunctional exploration of the central nervous system. ElectromyographyClinical and neurophysiological evaluation of neuromuscular pathology.
ElectromyographyClinical and neurophysiological evaluation of neuromuscular pathology. DensitometryDiagnostic technique for checking bone mineral density.
DensitometryDiagnostic technique for checking bone mineral density. UrodynamicsDiagnosis of urination disorders and incontinence.
UrodynamicsDiagnosis of urination disorders and incontinence.
- Chequeos médicos

 GeneralUn control inteligente de tu salud
GeneralUn control inteligente de tu salud CompletoUn examen exhaustivo de tu salud
CompletoUn examen exhaustivo de tu salud Completo PlusNuestro chequeo más exclusivo
Completo PlusNuestro chequeo más exclusivo ViajerosSi vas a emprender un viaje, tu salud es parte del equipaje
ViajerosSi vas a emprender un viaje, tu salud es parte del equipaje DeportivoUna revisión a fondo para potenciar tu rendimiento
DeportivoUna revisión a fondo para potenciar tu rendimiento CardiológicoUna buena noticia es saber que tu corazón está bajo control
CardiológicoUna buena noticia es saber que tu corazón está bajo control Para empresasUna herramienta que potencia la satisfacción, productividad y fidelización del empleado
Para empresasUna herramienta que potencia la satisfacción, productividad y fidelización del empleado
- Diagnostic tests
- Our centre
- Teknon Healthcare Service Areas
 InpatientBright, functional and fully equipped rooms.
InpatientBright, functional and fully equipped rooms. Semi-critical Care UnitEquipped with technology for diagnoses and treatments that require special care.
Semi-critical Care UnitEquipped with technology for diagnoses and treatments that require special care. Healthy Nutrition ProgrammeWe want to improve people’s health, which is why we promote healthy, conscious and sustainable nutrition at our hospitals.
Healthy Nutrition ProgrammeWe want to improve people’s health, which is why we promote healthy, conscious and sustainable nutrition at our hospitals. NursingOver 400 professionals.
NursingOver 400 professionals. Emergency DepartmentUninterrupted operation, 24/7 at your service.
Emergency DepartmentUninterrupted operation, 24/7 at your service. Exclusivity / Teknon ClubCommitted to superior and individualised service, we furnish a full range of services in conjunction with our medical and healthcare support.
Exclusivity / Teknon ClubCommitted to superior and individualised service, we furnish a full range of services in conjunction with our medical and healthcare support. Surgical AreaA total of twenty (20) operating theatres, 12 of which are equipped for high-risk surgery.
Surgical AreaA total of twenty (20) operating theatres, 12 of which are equipped for high-risk surgery. International ProgrammeA programme agent will provide you with comprehensive, personalised support
International ProgrammeA programme agent will provide you with comprehensive, personalised support Healthcare Ethics CommitteeGuidance for citizens and professionals in cases of moral conflicts.
Healthcare Ethics CommitteeGuidance for citizens and professionals in cases of moral conflicts. ICU-CCUMultipurpose unit incorporating treatment cubicles equipped with modern monitoring systems.
ICU-CCUMultipurpose unit incorporating treatment cubicles equipped with modern monitoring systems. Patient servicesAvailable to all our patients and their companions.
Patient servicesAvailable to all our patients and their companions. ResearchResearch is one of the cornerstones of Centro Médico Teknon.
ResearchResearch is one of the cornerstones of Centro Médico Teknon. Programa de Seguimiento PersonalizadoTe acompañamos durante tu proceso médico. Organizamos y agendamos tus citas y pruebas.
Programa de Seguimiento PersonalizadoTe acompañamos durante tu proceso médico. Organizamos y agendamos tus citas y pruebas. Calidad y Seguridad del PacienteAdoptamos modelos de gestión basados en los estándares más exigentes nacionales e internacionales.
Calidad y Seguridad del PacienteAdoptamos modelos de gestión basados en los estándares más exigentes nacionales e internacionales.
- Teknon Healthcare Service Areas
- News
- Actualidad
 NoticiasConoce qué está pasando en Centro Médico Teknon. Consulta nuestra sección de noticias.
NoticiasConoce qué está pasando en Centro Médico Teknon. Consulta nuestra sección de noticias. AgendaPuedes encontrar todos los eventos que hemos organizado sobre salud y aquellos temas de actualidad que te pueden interesar. Accede a nuestra agenda de actividades.
AgendaPuedes encontrar todos los eventos que hemos organizado sobre salud y aquellos temas de actualidad que te pueden interesar. Accede a nuestra agenda de actividades. VídeosEn esta sección encontrarás una amplia colección de videos relacionados con nuestras especialidades.
VídeosEn esta sección encontrarás una amplia colección de videos relacionados con nuestras especialidades. PodcastTemas médicos de actualidad, tratamientos innovadores, consejos de salud y experiencias de pacientes abordados por nuestros especialistas.
PodcastTemas médicos de actualidad, tratamientos innovadores, consejos de salud y experiencias de pacientes abordados por nuestros especialistas. Contenidos de salud
Contenidos de salud
- Actualidad
- Blog

- Medical directory
- Specialities
- Unidades especializadas
- Instituto del Corazón
- Unidad de Obesidad
- Instituto Oncológico
- Unidad de Medicina y Cirugía sin sangre
- Instituto de Neurociencias
- Unidad de Atención al Lesionado de Tráfico
- Instituto de Neumología
- Unidad de Medicina Marítima
- Instituto de Terapia Regenerativa Tisular
- Unidad de Tratamiento del Dolor
- Clínica del Tenis
- Unidad de Enfermedades Inflamatorias y Autoinmunes
- Unidad de Reproducción
Asistida
- Unidad del Sueño
- Unidad de Síndromes de Sensibilización Central
- Unidades especializadas
- Diagnostics
- Diagnostic tests
- Diagnostic ImagingDiagnostic and interventional scans.
- Anatomical pathology laboratoryAllows to obtain a second opinion from renowned specialists.
- Clinical Analysis LaboratoryComprehensive service in the clinical area.
- EndoscopyAn accurate diagnosis without conventional surgery.
- ElectrophysiologyFunctional exploration of the central nervous system.
- ElectromyographyClinical and neurophysiological evaluation of neuromuscular pathology.
- DensitometryDiagnostic technique for checking bone mineral density.
- UrodynamicsDiagnosis of urination disorders and incontinence.
- Chequeos médicos
- GeneralUn control inteligente de tu salud
- CompletoUn examen exhaustivo de tu salud
- Completo PlusNuestro chequeo más exclusivo
- ViajerosSi vas a emprender un viaje, tu salud es parte del equipaje
- DeportivoUna revisión a fondo para potenciar tu rendimiento
- CardiológicoUna buena noticia es saber que tu corazón está bajo control
- Para empresasUna herramienta que potencia la satisfacción, productividad y fidelización del empleado
- Diagnostic tests
- Our centre
- Teknon Healthcare Service Areas
- InpatientBright, functional and fully equipped rooms.
- Semi-critical Care UnitEquipped with technology for diagnoses and treatments that require special care.
- Healthy Nutrition ProgrammeWe want to improve people’s health, which is why we promote healthy, conscious and sustainable nutrition at our hospitals.
- NursingOver 400 professionals.
- Emergency DepartmentUninterrupted operation, 24/7 at your service.
- Exclusivity / Teknon ClubCommitted to superior and individualised service, we furnish a full range of services in conjunction with our medical and healthcare support.
- Surgical AreaA total of twenty (20) operating theatres, 12 of which are equipped for high-risk surgery.
- International ProgrammeA programme agent will provide you with comprehensive, personalised support
- Healthcare Ethics CommitteeGuidance for citizens and professionals in cases of moral conflicts.
- ICU-CCUMultipurpose unit incorporating treatment cubicles equipped with modern monitoring systems.
- Patient servicesAvailable to all our patients and their companions.
- ResearchResearch is one of the cornerstones of Centro Médico Teknon.
- Programa de Seguimiento PersonalizadoTe acompañamos durante tu proceso médico. Organizamos y agendamos tus citas y pruebas.
- Calidad y Seguridad del PacienteAdoptamos modelos de gestión basados en los estándares más exigentes nacionales e internacionales.
- Teknon Healthcare Service Areas
- News
- Actualidad
- NoticiasConoce qué está pasando en Centro Médico Teknon. Consulta nuestra sección de noticias.
- AgendaPuedes encontrar todos los eventos que hemos organizado sobre salud y aquellos temas de actualidad que te pueden interesar. Accede a nuestra agenda de actividades.
- VídeosEn esta sección encontrarás una amplia colección de videos relacionados con nuestras especialidades.
- PodcastTemas médicos de actualidad, tratamientos innovadores, consejos de salud y experiencias de pacientes abordados por nuestros especialistas.
- Contenidos de salud
- Actualidad
- Blog

- Especialidades
 Bardají Bofill Manel
Bardají Bofill Manel- Servicios
- Hernia
- Inguinal hernia
- Hernioplastia según la técnica de rutkow-Robbins



 Inguinal Hernia Repair with cone placement Hernioplasty according to rutkow-Robbins technique, consists of a technique in which a cone (Perfix Plug) of polypropylene is used, which is recommended for the repair of any type of inguinal hernia either primary or recurrent, direct or indirect, giving significant advances, compared to the conventional technique (by suture), It does not require so much dissection of the tissues and at the same time being this a "tension-free" technique. This results in decreased postoperative pain, faster rehabilitation and a lower rate of recurrences (less than 1%).
Inguinal Hernia Repair with cone placement Hernioplasty according to rutkow-Robbins technique, consists of a technique in which a cone (Perfix Plug) of polypropylene is used, which is recommended for the repair of any type of inguinal hernia either primary or recurrent, direct or indirect, giving significant advances, compared to the conventional technique (by suture), It does not require so much dissection of the tissues and at the same time being this a "tension-free" technique. This results in decreased postoperative pain, faster rehabilitation and a lower rate of recurrences (less than 1%).
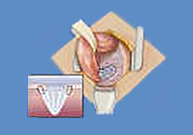
The surgery takes an average of 25 minutes or less to perform, thus offering a time-cost savings. The shape of the apex of the cone facilitates insertion into the hernia defect, while the pre-formed "petals" conform to the anatomy of the inguinal canal. This design minimizes any need to adapt.
The entire operation takes less time from incision to cone placement. The plug-coupling technique is simplistic, in standardized form, since it can be used in the repair of virtually any inguinal hernia.
The peritoneal cavity is not entered and there is no ileus or postoperative nausea. Patients have less pain and decreasing the amount of dissection decreases blood loss.
From January 1989 to June 1997, Drs. Robbins and Rutkow performed 3,152 inguinal plasties with this technique, of which 88% were primary and the remaining 12% were recurrent, obtaining results of 1% of recurrences in the first and 2% in the second group. In contrast to traditional techniques where a recurrence of up to 10 to 15% is observed.
The type of anesthesia required is local or regional, the patient can return a few hours after surgery, also the patient can start some type of slight effort the next day. In general, most patients can perform their normal activities by the end of the second or third week.
There are many patients who have inguinal hernia, who do not accept or seek the help of the doctor for fear of pain or disability, today more patients have undergone surgery with this technique, favoring the approach of patients.
Arthur I. Gilbert technique
The Sutureless Repair Technique is based on three concepts:
- IIA is an appropriate passage to the retromuscular preperitoneal space
- The mesh is an adequate and effective barrier 3. the body's own forces are sufficient to ensure repair (Pascal's principle)
Directions
- Indirect hernias type I-II (with deep inguinal opening (OIP) less than 4 cm)
- In some primary and recurrent hernias
Technique
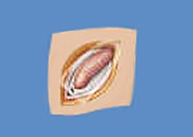
- Evaluation of the internal inguinal ring. It requires a high dissection of the sac to invaginate it in the preperitoneal space. With a finger on the OIP, its size is checked and the hernia is classified. All types I, II and III can be susceptible to this technique.
- Mesh. The right size for preparing the mesh should be 6 x 6 cm. It is cut from the middle of one side to the center of the mesh and bent successively rotating it 90º each time to form a stopper in paraguas.
- Collocation. It is inserted through the OIP to be placed between the peritoneum and the fascia transversalis. In the preperitoneal space the paragüas opens and adapts to the ring without fixation. Subsequently, the patient is asked to perform a Valsalva maneuver to check its correct position and integrity of the sphincter mechanism.
- Subsequent reinforcement. The posterior wall is reinforced by placing without suture a second extended mesh of 6 x 4 cm, sectioned laterally to make way for the cord (Figure 2).
Technique by Ira M. Rutkow
It is based on the principle that repair by means of a mesh plug (which is preferable to an extended mesh) is always an effective treatment whatever the existing defect (3).
Directions
The author advises this technique in all inguinocrural hernias based on the axiom "the lower the dissection, the better the results".
Technique
- Mesh: The cap is formed as in the Gilbert technique but its size must accommodate the existing defect.
- Fixation: varies according to the type of hernia.
- Type I. No suture is ever required.
- Type II. It usually does not require suturing. The decision to use stitches is up to the surgeon.
- Type III. The cone is always fixed to the margins of the hernial orifice with several resorbable loose points.
- Type IV and V. The direct defect is circumscribed near its base with electrocautery to leave a visible margin around the healthy tissue, and then the hernia is reduced. The plug is inserted through the posterior defect and fixed. (Figure 3).
- Type VI or in pants. Two plugs may occasionally be required.
- A Valsalva maneuver should always be performed afterwards to evaluate its correct position.
- Posterior reinforcement: in all cases a second reinforcement mesh without suture is placed. The lateral section to make way for the cord is closed with 2 loose stitches.