

- Medical directory
- Specialities
- Specialised Units
 Teknon Cardiology Institute
Teknon Cardiology Institute Obesity Unit
Obesity Unit Teknon Oncology Institute
Teknon Oncology Institute Bloodless Medicine and Surgery Unit
Bloodless Medicine and Surgery Unit Teknon Institute of Neurosciences
Teknon Institute of Neurosciences Traffic Accident Care Unit
Traffic Accident Care Unit Teknon Pulmonology Unit
Teknon Pulmonology Unit Maritime Medicine Unit
Maritime Medicine Unit Institute of Tissue Regenerative Therapy
Institute of Tissue Regenerative Therapy Teknon Pain Treatment Unit
Teknon Pain Treatment Unit Teknon Tennis Clinic
Teknon Tennis Clinic Systemic Inflammatory and Autoimmune Diseases Unit
Systemic Inflammatory and Autoimmune Diseases Unit Assisted Reproduction Unit
Assisted Reproduction Unit Sleep Unit
Sleep Unit Unidad de Síndromes de Sensibilización Central
Unidad de Síndromes de Sensibilización Central
- Specialised Units
- Diagnostics
- Diagnostic tests
 Diagnostic ImagingDiagnostic and interventional scans.
Diagnostic ImagingDiagnostic and interventional scans. Anatomical pathology laboratoryAllows to obtain a second opinion from renowned specialists.
Anatomical pathology laboratoryAllows to obtain a second opinion from renowned specialists. Clinical Analysis LaboratoryComprehensive service in the clinical area.
Clinical Analysis LaboratoryComprehensive service in the clinical area. EndoscopyAn accurate diagnosis without conventional surgery.
EndoscopyAn accurate diagnosis without conventional surgery. ElectrophysiologyFunctional exploration of the central nervous system.
ElectrophysiologyFunctional exploration of the central nervous system. ElectromyographyClinical and neurophysiological evaluation of neuromuscular pathology.
ElectromyographyClinical and neurophysiological evaluation of neuromuscular pathology. DensitometryDiagnostic technique for checking bone mineral density.
DensitometryDiagnostic technique for checking bone mineral density. UrodynamicsDiagnosis of urination disorders and incontinence.
UrodynamicsDiagnosis of urination disorders and incontinence.
- Medical check-ups

 GeneralThe most intelligent health check-up
GeneralThe most intelligent health check-up FullA comprehensive examination of your health
FullA comprehensive examination of your health Full PlusOur most exclusive check-up
Full PlusOur most exclusive check-up TravellersWhen travelling, your health is also part of your luggage
TravellersWhen travelling, your health is also part of your luggage SportA thorough review to boost your performance
SportA thorough review to boost your performance CardiologyGood news is knowing your heart is under control
CardiologyGood news is knowing your heart is under control For companiesA tool that enhances employee satisfaction, productivity, and loyalty
For companiesA tool that enhances employee satisfaction, productivity, and loyalty
- Diagnostic tests
- Our centre
- Teknon Healthcare Service Areas
 InpatientBright, functional and fully equipped rooms.
InpatientBright, functional and fully equipped rooms. Semi-critical Care UnitEquipped with technology for diagnoses and treatments that require special care.
Semi-critical Care UnitEquipped with technology for diagnoses and treatments that require special care. Healthy Nutrition ProgrammeWe want to improve people’s health, which is why we promote healthy, conscious and sustainable nutrition at our hospitals.
Healthy Nutrition ProgrammeWe want to improve people’s health, which is why we promote healthy, conscious and sustainable nutrition at our hospitals. NursingOver 400 professionals.
NursingOver 400 professionals. Emergency DepartmentUninterrupted operation, 24/7 at your service.
Emergency DepartmentUninterrupted operation, 24/7 at your service. Exclusivity / Teknon ClubCommitted to superior and individualised service, we furnish a full range of services in conjunction with our medical and healthcare support.
Exclusivity / Teknon ClubCommitted to superior and individualised service, we furnish a full range of services in conjunction with our medical and healthcare support. Surgical AreaA total of twenty (20) operating theatres, 12 of which are equipped for high-risk surgery.
Surgical AreaA total of twenty (20) operating theatres, 12 of which are equipped for high-risk surgery. International ProgrammeA programme agent will provide you with comprehensive, personalised support
International ProgrammeA programme agent will provide you with comprehensive, personalised support Healthcare Ethics CommitteeGuidance for citizens and professionals in cases of moral conflicts.
Healthcare Ethics CommitteeGuidance for citizens and professionals in cases of moral conflicts. ICU-CCUMultipurpose unit incorporating treatment cubicles equipped with modern monitoring systems.
ICU-CCUMultipurpose unit incorporating treatment cubicles equipped with modern monitoring systems. Patient servicesAvailable to all our patients and their companions.
Patient servicesAvailable to all our patients and their companions. ResearchResearch is one of the cornerstones of Centro Médico Teknon.
ResearchResearch is one of the cornerstones of Centro Médico Teknon. Personalised Follow-up ProgrammeWe accompany you throughout your medical journey. We organise your appointments and tests.
Personalised Follow-up ProgrammeWe accompany you throughout your medical journey. We organise your appointments and tests. Patient Quality and SafetyOur management models are based on the most stringent national and international standards.
Patient Quality and SafetyOur management models are based on the most stringent national and international standards.
- Teknon Healthcare Service Areas
- News
- News
 NewsKeep abreast of the events at Centro Médico Teknon. Visit our News section.
NewsKeep abreast of the events at Centro Médico Teknon. Visit our News section. AgendaHere we post upcoming events and discussions on relevant health topics. Visit our Agenda section to see what’s up.
AgendaHere we post upcoming events and discussions on relevant health topics. Visit our Agenda section to see what’s up. VideosThis section contains an extensive collection of videos related to our specialities.
VideosThis section contains an extensive collection of videos related to our specialities. PodcastOur specialists discuss current medical topics, innovative treatments, health advice and patient experience.
PodcastOur specialists discuss current medical topics, innovative treatments, health advice and patient experience. Health content
Health content
- News
- Blog

- Medical directory
- Specialities
- Specialised Units
- Teknon Cardiology Institute
- Obesity Unit
- Teknon Oncology Institute
- Bloodless Medicine and Surgery Unit
- Teknon Institute of Neurosciences
- Traffic Accident Care Unit
- Teknon Pulmonology Unit
- Maritime Medicine Unit
- Institute of Tissue Regenerative Therapy
- Teknon Pain Treatment Unit
- Teknon Tennis Clinic
- Systemic Inflammatory and Autoimmune Diseases Unit
- Assisted Reproduction Unit
- Sleep Unit
- Unidad de Síndromes de Sensibilización Central
- Specialised Units
- Diagnostics
- Diagnostic tests
- Diagnostic ImagingDiagnostic and interventional scans.
- Anatomical pathology laboratoryAllows to obtain a second opinion from renowned specialists.
- Clinical Analysis LaboratoryComprehensive service in the clinical area.
- EndoscopyAn accurate diagnosis without conventional surgery.
- ElectrophysiologyFunctional exploration of the central nervous system.
- ElectromyographyClinical and neurophysiological evaluation of neuromuscular pathology.
- DensitometryDiagnostic technique for checking bone mineral density.
- UrodynamicsDiagnosis of urination disorders and incontinence.
- Medical check-ups
- GeneralThe most intelligent health check-up
- FullA comprehensive examination of your health
- Full PlusOur most exclusive check-up
- TravellersWhen travelling, your health is also part of your luggage
- SportA thorough review to boost your performance
- CardiologyGood news is knowing your heart is under control
- For companiesA tool that enhances employee satisfaction, productivity, and loyalty
- Diagnostic tests
- Our centre
- Teknon Healthcare Service Areas
- InpatientBright, functional and fully equipped rooms.
- Semi-critical Care UnitEquipped with technology for diagnoses and treatments that require special care.
- Healthy Nutrition ProgrammeWe want to improve people’s health, which is why we promote healthy, conscious and sustainable nutrition at our hospitals.
- NursingOver 400 professionals.
- Emergency DepartmentUninterrupted operation, 24/7 at your service.
- Exclusivity / Teknon ClubCommitted to superior and individualised service, we furnish a full range of services in conjunction with our medical and healthcare support.
- Surgical AreaA total of twenty (20) operating theatres, 12 of which are equipped for high-risk surgery.
- International ProgrammeA programme agent will provide you with comprehensive, personalised support
- Healthcare Ethics CommitteeGuidance for citizens and professionals in cases of moral conflicts.
- ICU-CCUMultipurpose unit incorporating treatment cubicles equipped with modern monitoring systems.
- Patient servicesAvailable to all our patients and their companions.
- ResearchResearch is one of the cornerstones of Centro Médico Teknon.
- Personalised Follow-up ProgrammeWe accompany you throughout your medical journey. We organise your appointments and tests.
- Patient Quality and SafetyOur management models are based on the most stringent national and international standards.
- Teknon Healthcare Service Areas
- News
- News
- NewsKeep abreast of the events at Centro Médico Teknon. Visit our News section.
- AgendaHere we post upcoming events and discussions on relevant health topics. Visit our Agenda section to see what’s up.
- VideosThis section contains an extensive collection of videos related to our specialities.
- PodcastOur specialists discuss current medical topics, innovative treatments, health advice and patient experience.
- Health content
- News
- Blog


- Specialised Units
 Diagnostic tests
Diagnostic tests- Treatments and Specialities
- Endoscopy
- Barrett's oesophagus
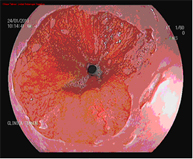
Barrett's oesophagus
Barrett's oesophagus occurs when the epithelium (the outermost layer of the oesophageal wall) is replaced by another type of epithelium containing intestinal-type cells as a result of ongoing damage from gastroesophageal reflux (which is usually acidic), a condition known as intestinal metaplasia.
There are different types or grades of Barrett's oesophagus, according to the biopsy results and microscopic study. The grades can be:
- Intestinal metaplasia without dysplasia
- Intestinal metaplasia with low-grade dysplasia
- Intestinal metaplasia with high-grade dysplasia
Dysplasia refers to the inherent alterations of a tissue or cell, making it more disorganised and similar to a cancerous cell. Although dysplasia increases cancer risk, it is not considered cancer itself but rather a precancerous lesion. Ultimately, high-grade dysplasia may be considered cancer if there are signs of tissue invasion. As there is a risk of developing oesophageal cancer, it is very important to identify patients with this condition, make an accurate diagnosis, and establish the most precise and effective treatment. That is why our patients have access to the Barrett's Oesophagus Unit, made up of specialists offering the most accurate diagnosis and treatment, as well as the most innovative techniques.
What are the risks for a patient with Barrett's oesophagus?
Barrett’s oesophagus increases the risk of developing oesophageal adenocarcinoma (a specific type of cancer). Although all grades of Barrett’s oesophagus increase the patient’s risk compared to the general population, low- and high-grade dysplasia present the greatest risk.
| DIAGNOSIS | % risk per year | % risk in 4 years |
| Advanced intestinal metaplasia with low-grade dysplasia | 4.3% | 16.1% |
| Advanced intestinal metaplasia with high-grade dysplasia | 0.9% | 3.6% |
| Advanced intestinal metaplasia in oesophageal cancer | 0.5% | 2.0% |
*Data source: Sharma P, Falk GW, Weston AP, et al.
Dysplasia and cancer in a large multicenter cohort of patients with Barrett's esophagus.
Clin Gastroenterol Hepatol 2006; 4:566-572.
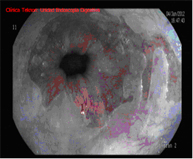
How is diagnosis performed?
Diagnosis is performed using high-resolution magnification endoscopy (image enhancement), employing additional chromoendoscopy techniques conducted by endoscopists specialised in the early diagnosis of premalignant lesions, with targeted biopsies for analysis.


When should Barrett's oesophagus be treated and which technique is indicated in each case?
Barrett's oesophagus should currently only be treated when dysplasia appears and is maintained or confirmed in a follow-up at 3-6 months (depending on the degree of dysplasia), with radiofrequency being the technique of choice if there are no visible lesions. Mucosectomy followed by radiofrequency on the remaining Barrett's oesophagus is the technique of choice if these lesions exist.
Treating Barrett's oesophagus involves controlling acid or gastroesophageal reflux to prevent it from progressing. High-dose treatment with acid production inhibitors is the treatment of choice, with antireflux surgery being considered as an alternative.

Endoscopic Techniques for the Treatment of Barrett's Oesophagus
Endoscopic mucosectomy
Endoscopic mucosal resection involves the endoscopic removal of a section of the mucosa and submucosa (in this case of the oesophagus). It is indicated whenever elevated lesions are observed in Barrett's oesophagus during diagnostic endoscopy.
This diagnostic test is conducted on an outpatient basis, with patients remaining under observation in the day hospital for a few hours.
Radiofrequency with HALO system
The HALO radiofrequency ablation system safely and uniformly ablates the oesophageal mucosa to a depth of approximately 1 mm. Ablation is a technique in which tissue is heated until it is no longer viable or alive. HALO technology is a very specific type of ablation where heat energy is applied precisely and in a controlled manner. Clinical trials have demonstrated that Barrett's tissue can be completely eliminated with HALO ablation technology in 98.4% of patients.
Endoscopic follow-up is required, and treatment generally needs to be repeated in one or two sessions.
How should Barrett's oesophagus be monitored?
An initial endoscopy with biopsies should be performed following the Seattle protocol. An endoscopic checkup is recommended after one year if there is no dysplasia but Barrett’s oesophagus is present, simultaneously increasing the dose of the gastric protector or its derivatives and ensuring complete inhibition of acid reflux through pH monitoring.
An endoscopic check is performed every 2-3 years if the second endoscopy still shows no dysplasia and the acid is controlled.
Endoscopic treatment is indicated whenever dysplasia is confirmed in a second checkup.